Implantable Collamer Lens
Also known as ICL
Medical Disclaimer: Information on this page is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.
See our Terms and Telemedicine Consent for details.

Overview
An Implantable Collamer Lens (ICL) is a clear, flexible lens that is gently tucked behind your iris and in front of the natural lens to correct blurry distance vision caused by moderate-to-high nearsightedness and astigmatism. Unlike LASIK, no corneal tissue is removed, and the lens can be removed later if your needs change. The American Academy of Ophthalmology notes that today’s EVO ICL design includes a microscopic central port that lets fluid circulate freely, eliminating the need for a pre-op laser iridotomy.1 The U.S. Food & Drug Administration cleared the latest EVO/EVO+ Visian ICL family in 2022 for prescriptions up to –20 D of myopia and 4 D of astigmatism.2
How the Procedure Works & Options
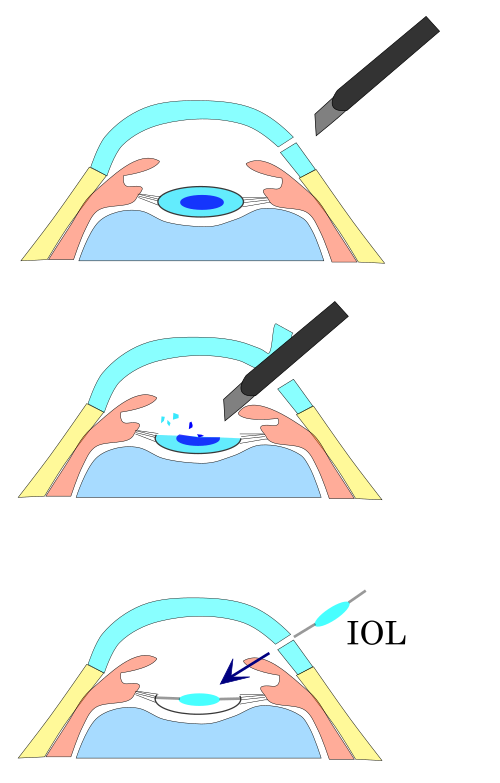
The outpatient surgery takes about 15 minutes per eye. After numbing drops, the surgeon makes a 3 mm self-sealing incision at the corneal edge, folds the ICL inside a tiny cartridge, and slides it through the incision into the posterior chamber. Special forceps unfold and center the lens so its four flexible corners rest in the ciliary sulcus, safely vaulting over the natural lens. New models have built-in toric power for astigmatism, and an EVO+ version offers a wider optical zone for large pupils.1 Cleveland Clinic reminds patients that no stitches are required and both eyes are often treated the same day.3
Who Is a Candidate?
Good candidates are adults 21–45 whose prescriptions have changed less than 0.5 D in a year, have healthy eyes, and an anterior-chamber depth of at least 3.0 mm from the cornea to the natural lens. ICLs shine when laser vision-correction is limited—very high myopia (–8 D to –20 D), thin or irregular corneas, dry-eye risk, or contact-sport lifestyles. A 2024 prospective study confirmed excellent safety even in eyes with relatively shallow chambers when the vault and sizing are calculated carefully.4 People with active uveitis, uncontrolled glaucoma, or low endothelial cell counts are generally deferred.1
ICL Suitability Score
Select your details to estimate suitability.
Cost and Price
ICL surgery is considered elective and is rarely covered by insurance. In the United States the typical package—including pre-op tests, the lens, surgery, and one-year follow-up—runs $3,500 – $5,500 per eye. Cleveland Clinic’s patient guide cites national averages near $4,000 per eye.3 NVISION Eye Centers list a range of $1,500 – $5,000 depending on geography, surgeon experience, and lens model, with many practices offering 0 % financing or HSA/FSA payment plans.7
Benefits and Limitations
Benefits: Over 95 % of eyes reach 20/20 or better, vision is often clear within 24 hours, and the lens material filters UV light. A five-year AAO Editors’ Choice review reported stable refraction, high patient satisfaction, and a low 0.6 % rate of significant cataract.8 Limitations & risks: rare night halos, the need for lifelong eye checks, and potential complications such as elevated eye pressure or cataract. A 2025 Frontiers analysis of FDA MAUDE data found serious adverse-event reporting at roughly 0.2 % of implanted lenses, with most events manageable by early detection.5
Recovery and Long-Term Care
You go home the same day wearing a clear shield. Antibiotic and steroid drops are used four times daily for one week, then tapered. Many people drive the next morning and return to desk work within 48 hours. Swimming, eye make-up, and heavy lifting wait one to two weeks. Follow-up visits are scheduled at day 1, week 1, month 1, then every six to 12 months to monitor lens vault, eye pressure, and corneal endothelial cells.31
Latest Research & Innovations
Next-generation “EVO Viva” lenses aim to add reading power for early presbyopia, while lab work explores drug-eluting ICLs to prevent inflammation. A 2024 real-world analysis of 2,300 FDA adverse-event reports showed no signal of unexpected risks and endorsed the value of the central-port design for pressure control.5 Ten-year follow-up data presented at ARVO demonstrated 93 % lens retention without visually significant cataract, reinforcing long-term safety for high myopes.9
Recent Peer-Reviewed Research
Efficacy of small incision lenticule extraction (SMILE), femtosecond-assisted laser in situ keratomileusis (FS-LASIK), and toric implantable collamer lens (TICL) implantation in correcting myopia with high astigmatism: a vector analysis.
Jiao X, Xue W, Zhou Z, et al.
A Comparison of Predicted and Achieved Postoperative Vaults in Implantable Collamer Lenses in White and Asian Eyes.
Ashton CBJ, Hammer A, Heeren TFC, et al.
Intraoperative OCT Enables Prediction of 3-Month Postoperative Lens Separation Vault for the Implantable Collamer Lens.
Reinstein MJB, Reinstein DZ, Archer TJ, et al.
Next Steps
If you’re highly nearsighted, have thin corneas, or simply want a reversible alternative to laser surgery, schedule a comprehensive refractive evaluation. A refractive lens specialist will measure your prescription, anterior-chamber depth, and endothelial cells to see whether the EVO ICL fits your eyes. You can connect with the right specialist on Kerbside for a medical-education consult—no physician-patient relationship will be created.17