Atropine Eye Drops for Myopia Control
Also known as Low-Dose Atropine, Myopia Control Drops
Medical Disclaimer: Information on this page is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.
See our Terms for details.


Overview
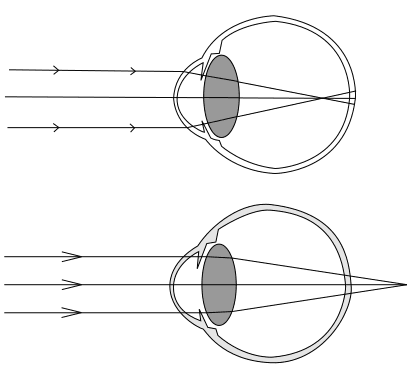
Low-dose atropine eye drops are nightly prescription drops used to help slow how quickly a child’s nearsightedness (myopia) gets worse. The medicine acts on the focusing system and signals the eye to grow more slowly, which can reduce year-to-year prescription changes. Parents like that the drop is easy to use, usually well tolerated, and fits into a bedtime routine. Professional groups describe low-dose atropine as an effective option for many children with progressing myopia. 1
Large clinical trials also show that some very low concentrations, like 0.01%, may not be strong enough to help, which is why dosing matters. 2
How the Procedure Works & Options
What it is: Atropine is an antimuscarinic medicine used in eye care for decades. For myopia control, doctors prescribe low concentrations (commonly 0.05%, 0.025%, or 0.01%) prepared by a licensed compounding pharmacy. One drop in each eye at bedtime is typical. Over months, the drops can slow axial eye growth and prescription change. The effect is dose-dependent in trials, with 0.05% often showing the strongest balance of benefit and comfort. 3
Important label notes: Commercial 1% atropine is FDA-approved for other eye uses (e.g., dilation), not specifically for myopia control; low-dose use is off-label. Labels list precautions such as light sensitivity and avoiding use in people at risk for narrow-angle glaucoma unless supervised. 5 Because compounding is involved, your clinician will select a trusted sterile pharmacy and provide storage and shelf-life guidance.
Who Is a Candidate?
Best fit: Children roughly ages 4–17 with progressive myopia (e.g., getting stronger by about ≥0.50 D per year) and otherwise healthy eyes. Kids with a family history of high myopia or with early, fast changes often benefit most. A complete exam confirms corneal health, eye pressure, pupil reactions, and rules out conditions where atropine is not advised. 9
Research suggests that 0.05% provides the most consistent slowing, with 0.025% offering moderate effect and 0.01% showing little to no benefit in some studies. 4
Cost and Price
How it’s supplied: Low-dose atropine is usually filled by a compounding pharmacy in 5–10 mL bottles, often lasting ~2–3 months with nightly dosing. In the U.S., typical cash prices are about $75–$120 per bottle; one example lists ~$95 for 10 mL (~90-day supply). 6
Because myopia control is off-label, insurance often does not cover the drops; ask your plan about exceptions. Many families use FSA/HSA funds for prescription eye medications, which can lower after-tax cost—see IRS Publication 502. 11
Smart budgeting tips:
- Request a written estimate (exam, axial-length measurements, medication, follow-ups).
- Ask about bottle size, beyond-use date (BUD), and storage; refrigerated bottles may last up to 90 days depending on the pharmacy.
- Compare local vs. mail-order compounders and confirm cold shipping if required.
- Set refill reminders so you don’t miss nightly doses.
Benefits and Limitations
Benefits: Randomized trials (LAMP) show that nightly low-dose atropine slows myopia progression and eye elongation in a dose-dependent way, with 0.05% generally performing best over three years and fewer lighting/reading side effects than historical high-dose drops. Meta-analyses also support overall effectiveness and safety in school-aged children.
Limits to know: 0.01% may not meaningfully slow myopia in many children, as shown in a U.S. randomized trial. 8 Benefits are greatest while drops are used consistently; stopping too early can allow faster progression to return, so your doctor will guide duration and any taper to reduce “rebound.” 7
Recovery and Long-Term Care
What your child may feel: Most kids see normally during the day. Some notice mild light sensitivity or slightly larger pupils in the morning, usually fading quickly—use sunglasses outdoors if needed. Rarely, a child may have near blur or headache at first; tell your clinician if this persists so the dose can be adjusted. 5
Follow-up: Expect checkups every 6–12 months for vision, prescription, and axial length. Plans often continue until eye growth slows (mid-teens), followed by a careful taper and monitoring for any rebound. Your doctor may also combine atropine with outdoor-time goals or optical methods based on age and progression. 7
Latest Research & Innovations
What studies show now: The LAMP program has followed children for multiple years and supports that 0.05% provides the strongest control among low doses, with guidance on when to continue, pause, or restart therapy. A network meta-analysis comparing many concentrations also ranks higher low-dose concentrations above very low ones for slowing eye growth. 12
Key nuance: Not all low doses are equal. The 0.01% U.S. trial did not beat placebo at two years, reminding families to pick a dose supported by stronger evidence and to individualize care. 8
Next Steps
If your child’s glasses get stronger each year, schedule a visit to discuss myopia control. A pediatric ophthalmologist or optometrist experienced in myopia management can confirm progression, measure axial length, and help choose a starting dose (often 0.05% or 0.025%) based on age, lifestyle, and side-effect tolerance. For plain-language background and FAQs, see the Academy’s patient page on atropine for myopia control. 7 To find a local Eye M.D., use the American Academy of Ophthalmology directory. 10